I am a speech language pathologist and instructor
of the standardized Kinesio® Taping curriculum. I thought
it would be helpful to put together a FAQ on Kinesio Taping®, specifically for speech
language pathologists!
WHAT IS THE KINESIO TAPING® STANDARDIZED
CURRICULUM?
The standardize Day 1, Day 2, and Day 3 are designed to teach
the following:
·
Day 1: The science behind Kinesio Tape® and its effects on systems of skin, periphery (nerves), fascia, muscles, joints, and circulatory/lymphatics
·
Day 2: Corrective techniques using specific cuts, tensions, and
applications with
Kinesio Tex Gold FPTM and Kinesio®
Tex Classic
·
Day 3: Kinesio Taping®- Clinical
analysis and applications (e.g., mixing/matching tape products/cuts to address
conditions with common etiologies)
·
All disciplines are required to take the same standardized curriculum. SLP/SLPA's are the only discipline required to take all three. This is due to ASHA bylaws on SLP/SLPA's being supervised, educated and certified to use medical modalities.
WHO CAN TAKE THE KINESIO TAPING® STANDARDIZED
CURRICULUM?
In order to attend a Kinesio Taping® seminar, each attendee must
meet all of the following criteria:
1. Must have completed 80 course hours of anatomy and physiology
2. Must have a working knowledge of the musculoskeletal system
3. Must be able to do assessments by evaluating and/or diagnosing
injuries and conditions.
4. Proof of completion of K1, 2 & 3 is required for KT4
participation.
5. Must have achieved or is a student in their junior or senior
year (transcripts must be provided) working towards one or more of the
following credentials: ARNP, ATC, CAT(C), CCSP, CDP, CHT, CLT, CMBT, CMT, CNMT,
COMT, COTA, COTA/L, CPO, CPT, CPTA, CRN, CST, CT, DC, DO, DOM, DPT, Lac, LAT,
LLCC, LMBT, LMP, LMT, LOT, LOTA, LPT, LPTA, MD, MDT, MLD, MOT, MOTR/L, MPT, MT,
MTC, NCMT, NCTMB, NDT, NMD, NMT, NP, NRC, OCS, ODT, OMD, OPA, OT, OTA, OTC,
OTR, OTR/L, PT, PT-C, PTA, PA, RMT, RN, RPT, RPTA, SLP/SLPA.
ARE CEU’S AWARDED FOR SPEECH LANGUAGE PATHOLOGISTS?
WHAT IS THE PROTOCOL TO USE IT CLINICALLY AS AN SLP/SLPA?
·
All SLP/SLPA participants must register for a Day 1-Day 3 block
session listed (all other disciplines can take Day 1-Day 2 only, with Day 3 and KT4 seminars being optional).
·
SLP/SLPA’s must take the certification class (Day 3) and pass the
exam to become certified to use Kinesio Tape® for clinical and billing
purposes.
·
Pre/post assessments will be administered for Day 1-Day 3
ARE THERE ANY KINESIO TAPING SEMINARS FOR
SPEECH RELATED AREAS?
Our KT4's are specialty classes. We are getting ready to launch
our newest KT 4 called "Microtaping applications for fragile populations
using Kinesio Tape). I am the lead author of this curriculum. It was also co-written
by my very good friend and colleague, Elizabeth G. Harvey, DPT, MSR, CKTI,
CEIM.
Here is the class description:
KT4 Specialty Class: Microtaping (MTA) applications for fragile
populations using Kinesio Tape®
(Prerequisite, completion of KINESIO UNIVERSITY approved Day 1-
Day 3 courses)
This course offers the participant taping strategies using smaller
cuts, lighter tensions, and specific taping products (Kinesio Tex Gold Light
Touch Plus (LT) and Kinesio Tex Classic Fan Cuts) to address postural
alignment, core stabilization, jaw stability, tongue control and lip mobility.
Also included are taping strategies to promote respiration, digestion, and scar
management. A new cut, the “Long and Short”, will be introduced for
multidirectional fascia release. The purpose of the class is to focus on
“minimal effective approaches” to promote function (e.g., alignment/stability,
balance, swallowing), skin integrity, and comfort for fragile populations
(e.g., infants, geriatric, neurologic populations (adult/ped). The participant
will be introduced to case studies, focusing on incorporating standardized
Kinesio taping applications with microtaping (MTA) applications.
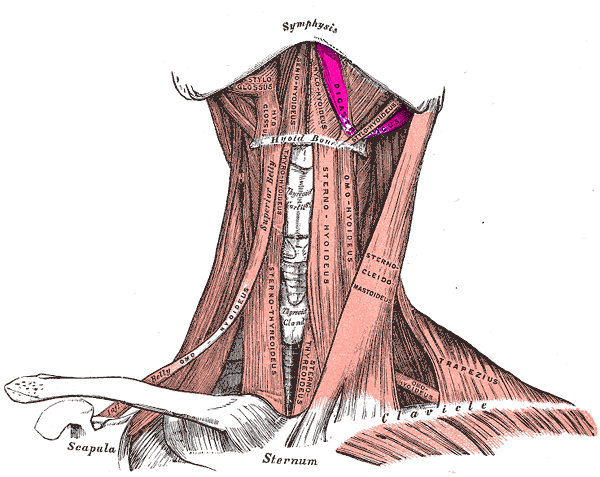
INFORMATION AND LITERATURE ON KINESIO TAPING® USED IN THE HEAD AND
NECK AREAS:
1.
S-tape
technique designed to address drooling
2.
The Clinical Effectiveness of Using Kinesio
Tape Following Wisdom Teeth Extraction. Henderson, Sarah Louise and Alexanders,
Jenny and Shaw, Thomas in Journal of Physiotherapy and Physical Rehabilitation
3.
Taping in the orofacial region.
4.
Effectiveness of Kinesiologic Taping Therapy in
Drooling Management among Children with Cerebral Palsy N=30 Aged 2-6
Romana Pervez, Ayesha Kamal But, Noreen
Tabassum
5.
Dr. Dwajee's study Lip tape therapy in patients
with a
cleft lip – a report on eight cases.
6.
The Kinesiology Taping as a method supporting
central
facial nerve damage (VII) therapy English
abstract only
Other studies:
1.
Does Elastic Therapeutic Tape Reduce Postoperative
Swelling, Pain, and Trismus After Open Reduction and Internal Fixation of
Mandibular Fractures?
2.
Kinesio Taping for temporomandibular
disorders: Single-blind, randomized, controlled trial of effectiveness
Disclaimer of Liability and WarrantyInformation presented in this blog is designed to promote ideas
and stimulate discussion. The goal of this blog is to provide a safe and
friendly place to share stories or experiences, build an understanding of various
teaching and treatment styles, and to network with each other.
The
author(s) of this blog do not dispense medical advice nor prescribe the use of information
as a form of treatment for medical problems with or without the advice of a
physician. The intent of the author(s) is only to offer information of a
general nature to help you cooperate with your doctor and clinical members in
your mutual quest for good health. In the event you use any of the information
in this blog for yourself, you are prescribing for yourself. The author(s)
assume no responsibility for your actions, assessment, nor interpretations. No
one associated with this blog will have liability for loss, damage, or injury,
resulting from the use of any information found on this or any other page at
this site.











{kind=link}
{kind=link}